Category
Ultrasound
Education
Year
2024
Clinicians sometimes say ‘air is the enemy of ultrasound’. Historically, clinicians avoided scanning the lungs, as air scatters ultrasound beams, resulting in artifacts and the inability to directly visualize lung tissue. However, astute clinicians quickly realized that artifacts can be a clue to important lung diseases. The diagnostic prowess of lung ultrasound has led to its adoption as a first-line tool for modern clinicians. So what are the core lung ultrasound artifacts we need to know? Let’s dive into A lines, B lines, Z lines and E lines!
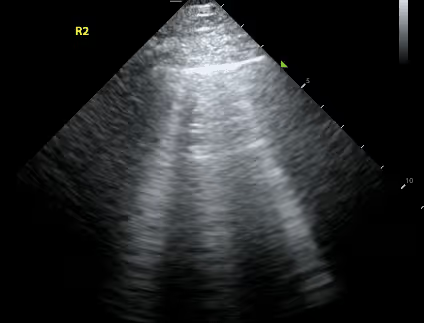
A lines are hyperechoic (ie. bright) horizontal lines that occur equidistant from the pleural line.

A lines are created by repetitive reflections between the pleural line and the ultrasound probe.
A lines are best seen when the transducer is positioned perpendicular to the lung surface. If you are unable to visualize them, you should tilt, rock or slide the probe to align the probe perpendicular to the curved lung.
The presence of A lines reflects normal lung (ie. lung that does not have pathology such as consolidation, pleural effusion or interstitial syndrome).
Note that A lines are still seen in pneumothorax.
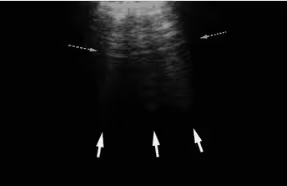
B lines are vertical hyperechoic artifacts originating from the pleural line that look similar to comet-tails. The artifact that generates B lines is the ‘ring down’ artifact.
B lines occur due to thickening of the interlobular septa, which are sheet-like structures that surround pulmonary lobules. Thickening can be due to fluid (eg. pulmonary edema, pulmonary hemorrhage), collagen fibrous tissue, or cells (eg. interstitial lung disease, sarcoidosis).
B lines are considered pathologic when there are three or more B lines in one rib space.
For a deeper dive into B lines, refer to our subsequent blog post here
Z lines are hyperechoic lines extending from the pleural line that can sometimes be mistaken for B line but are a common finding in normal lungs. There is no clinical significance to Z lines.
E lines are hyperechoic lines originating from air in the subcutaneous tissue that can sometimes be mistaken for B lines. One important feature of E lines is that they do not originate from the pleural line. Their presence may obscure adequate visualization of the pleural line.

Lung ultrasound has excellent diagnostic accuracy for a host of pulmonary pathology and its accurate interpretation requires an understanding of the most common lung ultrasound artifacts. For a more in depth dive, check out some of the references below and the Western Sono screencast on lung ultrasound found here.

Soni, N. J., Arntfield, R., & Kory, P. (2020). Point of care ultrasound. Elsevier. https://shop.elsevier.com/books/point-of-care-ultrasound/soni/978-0-323-54470-2
Radiology Key, Ultrasound Artifacts, accessed 13 November 2023, https://radiologykey.com/ultrasound-artifacts/.
Bhoil R, Ahluwalia A, Chopra R, Surya M, Bhoil S. Signs and lines in lung ultrasound. J Ultrason. 2021 Aug 16;21(86):e225-e233. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8439137/
Barile, Maria. (2020). Pulmonary Edema: A Pictorial Review of Imaging Manifestations and Current Understanding of Mechanisms of Disease. European Journal of Radiology Open. 7. https://www.ejropen.com/article/S2352-0477(20)30063-0/fulltext
Lichtenstein DA, Mezière GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest. 2008 Jul;134(1):117-25. doi: 10.1378/chest.07-2800. Epub 2008 Apr 10. Erratum in: Chest. 2013 Aug;144(2):721. https://journal.chestnet.org/article/S0012-3692(08)60155-5/abstract
Lichtenstein, Daniel & Meziere, Gilbert & Lagoueyte, Jean-François & Biderman, Philippe & Goldstein, Ivan & Gepner, Agnès. (2009). A-Lines and B-Lines Lung Ultrasound as a Bedside Tool for Predicting Pulmonary Artery Occlusion Pressure in the Critically III. Chest. 136. https://journal.chestnet.org/article/S0012-3692(09)60599-7/abstract
Francisco MJ Neto, Rahal A Junior, Vieira FA, Silva PS, Funari MB. Advances in lung ultrasound. Einstein (Sao Paulo). 2016 Jul-Sep;14(3):443-448. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5234763/


